
By
Marianna Wróbel
MSc Medical Anthropology
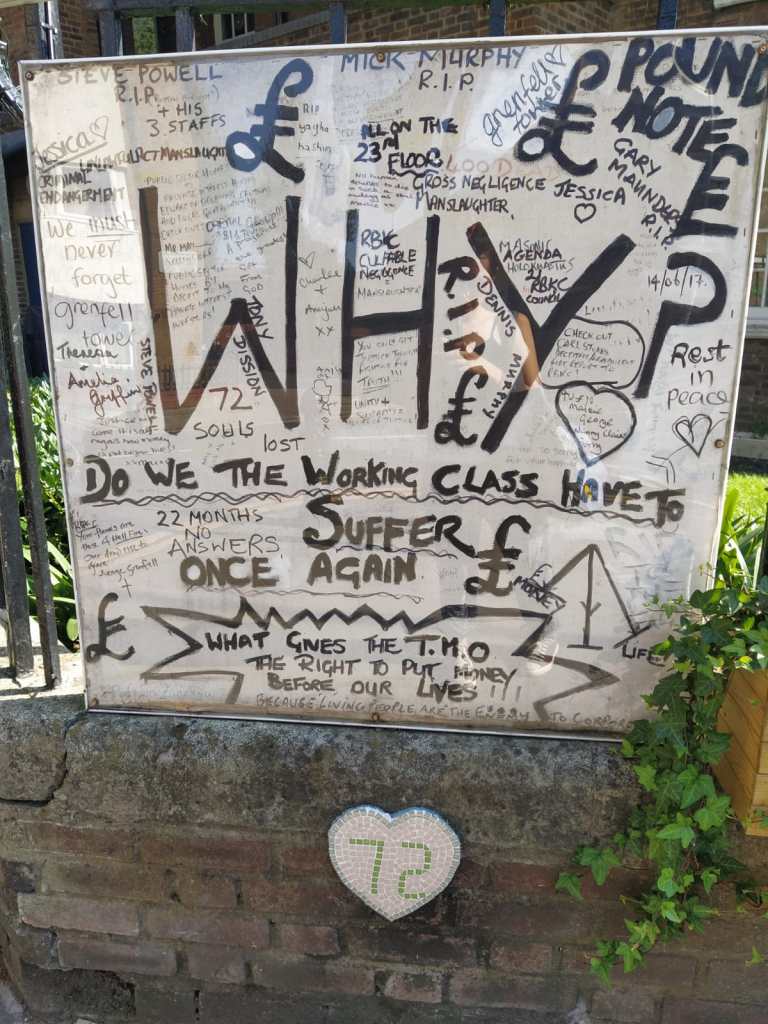
On June 14th, 2017 in one of the wealthiest boroughs of London – Kensington and Chelsea – Grenfell Tower, a 24-storey block of council flats, went on fire. It killed more than 80 people, leaving over 70 injured. The immediate cause given was an electrical fault in the refrigerator in one of the flats. However, as it was later established in the investigation, the fire spread so disastrously because of the flammable, exterior cladding. Evidence gathered disclosed that Grenfell Tower’s residents had contacted the building management multiple times to ask for fire risk assessment, or replacement of the faulty material, worried that cheap cladding might pose a serious risk, but to no avail. In the BBC documentary “Grenfell” the community members recall a day when they asked the building management if it were the cladding they would like to have on their house. The answer was short: “If I was getting it for nothing, I wouldn’t mind.” The investigation also revealed that the tower did not fulfil other fire safety requirements regarding sufficient fire exits and was not compliant with building regulations, a result of the council’s cost-cutting on social housing (Snow, 2018).
Immediately after the fire the whole community – including churches, mosque, and other religious organisations – came together to help the victims by providing them with food, clothes, and places to sleep. The community became the basis for living through the pain and grief, in the first minutes of the fire and long after it. However, the council officials did not show up: a fact emphasised by the survivors at every stage of the current investigation into the causes of the fire, on the walls of Notting Dale buildings, and by the organisations appointed by the survivors and families of the victims, Justice for Grenfell and Grenfell United. The help for the survivors was brought by the community volunteers, but no systematic or structural aid was provided. As Grenfell community members understand it, this abandonment in the most crucial moment was a symbolic refusal to share their pain; a clear border set between the two worlds (Keenan, 2019). In the long term, the feelings of betrayal grew significantly, as the council resources seemed to be inappropriately allocated: the “Wellbeing Centre” for those affected was built when what the Grenfell community said they needed was an investigation into the cause of the fire and removal of the harmful cladding in the towers still standing.
One year later an official report was published by the Royal Borough of Kensington and Chelsea that revealed that the proportion of the survivors and community members diagnosed with PTSD is unusually high. According to the NHS, typically one-third of people affected by a disaster are going to suffer from PTSD. In the case of Grenfell, it was 67% of those screened were diagnosed with the disorder; the number claimed to be significantly greater than in other post-disaster contexts (RBKC, 2018). Considerably, a high risk of secondary trauma was reported – of those indirectly affected, although not exposed to the fire itself. The report suggested that inhabitants of the tower were more prone to trauma as many of them have been of “poor mental health” before the fire due to financial struggles, their refugee status, or having many children (RBKC, 2018, p. 44). The council’s report concluded with the hope for further interrogation, perhaps through testing of the uncovered underlying mental problems of the community, and expressed its willingness to support its mental health through funding counselling, art therapy, or offering other forms of emotional support. The screenings, conducted by the NHS, ended with the establishment of the Grenfell Health and Wellbeing Centre at St Charles Hospital, close to Notting Dale, where further screenings for PTSD and Trauma-Focused Cognitive Behavioural Therapy are still offered. However, the approach that attributes high levels of PTSD to the refugee status or the difficult material conditions seems to omit the significance of how people with this socioeconomic status were perceived and treated by the authorities prior to the fire.
The overall of the Grenfell community’s experience with the council’s and city’s authorities fall into the politics of marginalisation, manifested as a chronic disaster syndrome (CDS). The term was used by Adams et al. (2009) to describe layers of suffering experienced on the individual, social and political level by the survivors of storm Katrina in New Orleans who suffered simultaneously from a traumatic experience of disaster, displacement, and government’s betrayal, rendering recovery impossible. It describes the individual suffering as a trauma of the particular event, but also looks at other phenomena of socioeconomic and political nature that are indistinguishable from the experience of the disaster itself. CDS manifests in the individual bodies as chronic distress and at the same time as the socioeconomic and sociocultural factors that produce suffering. This cluster of interrelated conditions effectively prevents recovery (Adams et al., 2009). A framework of CDS assumes a possibility of long-term instability and structural abandonment to exist as concurrently the cause, symptom, effect, and cure (ibid.) In the case of the Grenfell community, CDS displays as a life in a continuous state of “emergency” and insecurity rooted in enduring structural neglect, of which the Grenfell Tower fire was a disastrous result, and not a separate, “tragic” incident. A “tragedy” suggests an unforeseen, unprecedented event, inexplicable calamity beyond human comprehension, while the survivors argue that the Grenfell fire was to be expected as it was not merely an unfortunate turn of events without a human factor.

Almedom (2004), while working in a displaced person camp in Eritrea coined a model of psychosocial transition. She observed that outcome of a crisis on the mental health of the survivors and social cohesion depends on the level, type, and adequacy of available social support. Trauma, as a psychosocial category, might then be worsened, deepened, or alleviated depending on the response to suffering that survivors receive. In the Grenfell case, “trauma” used as a diagnostic and psychiatric category was addressed through the establishment of the wellbeing centre. However, the chronicity of marginalisation: the council’s lack of action before the fire, in the immediate aftermath and later, the fact that other buildings in the area to this day have the same flammable, poor quality cladding and not enough sufficient fire exits, and the overwhelming feeling of betrayal of the Grenfell residents were omitted in the public and psychiatric discourse. The establishment of the Grenfell Wellbeing Centre – the only large-scale investment in aid for the survivors of the fire – focused on only one, the individual aspect of chronic distress, ignoring all the conditions that produced it, and the terms such as “trauma” and “post-traumatic stress disorder” began to be used to describe the experience of the Grenfell fire survivors. Although CDS can be correlated with PTSD as chronic conditions of distress, it is more than that. Grenfell Wellbeing Centre, offering numerous counselling or bereavement services, was built in line with the standard psychiatric understanding of PTSD as a condition where symptoms are isolated in time and relate to the event in the past. The framework of CDS helps us understand the ongoing, continuous nature of suffering, insecurity, and feelings of abandonment that are rooted in the event before the disaster and flow to the present: the “war”, “fire” or any other disaster become physical manifestations of preceding, long-term experience, and recovery becomes possible when not only individual, but collective suffering and its causes are addressed.
Official narratives that constitute PTSD focus on the past rather than current events, appointing both victims and the perpetrators. The trauma of the Grenfell Tower fire undoubtedly persists in the individual lives of the Grenfell community. However, these events are present also as representations of the continuous struggle of people living in social housings that did not start and does not end with the fire. Social justice organisations established after the disaster such as Grenfell United and Justice for Grenfell do not accept the official and biomedical stories told of them as being the victims of the fire. They consider themselves to be the victims of what happened before, and, what is crucial, what happened after the Grenfell tower burned. Almedom’s (2004) model of “psychosocial transition” tells us that the wellbeing and recovery of the affected population depend on the response and aftermath manifested in the political dimension, not on the personal level of one’s mind. In that sense, recovery imagined through providing victims with exclusively bereavement support and PTSD therapies is an inadequate one, as long as the events that caused the disaster keep defining the presence of its victims (Adams et al., 2009). A true recovery would have to address years of neglect and encompass the radical structural change of the way people living in social housing are perceived and treated by the council and city officials.

- Adams V., T. van Hattum, and D. English (2009) Chronic Disaster Syndrome: Displacement, Disaster Capitalism, and the Eviction of the Poor from New Orleans. American Ethnologist 36(4):615-636.
- Almedom A. M. (2004) Factors that Mitigate War-Induced Anxiety and Mental Distress. Journal of Biosocial Science 36(4):445-461.
- Keenan, S. (2019) A Border in Every Street: Grenfell and the Hostile Environment. In D. Bulley, J. Edkins, and N. El-Enany (eds.) After Grenfell: Violence, Resistance, and Response. London: Pluto Press.
- Royal Borough of Kensington and Chelsea (RBKC) (2018) A Journey Of Recovery: Supporting Health and Wellbeing for the Communities Impacted by the Grenfell Tower Fire Disaster. Department of Public Health, London. Available at: https://cutt.ly/kyiZwD6 [Accessed 11 November 2020].
- Snow, J. (2018) Grenfell Tower: An Atrocity in Three Acts. In C. Armitstead (ed.) Tales of Two Londons: Stories from a Fractured City. London: OR Books.

A much needed perspective and an important insight into the prevalence of chronic disaster syndrome (CDS) among the surviving Grenfell Tower residents and community.
LikeLike